
Some nights, acid reflux feels like a second job. You prop yourself up with pillows, avoid late meals, keep antacids nearby, and still wake up with burning in your chest or a sour taste in your throat. By morning, you are tired, irritated, and wondering whether the VA will take this seriously.
If that sounds familiar, you are not overreacting. GERD can disrupt sleep, meals, work, exercise, and even the medications you can tolerate for other service-connected conditions. It also creates a lot of confusion in the disability process because many veterans heard one set of rules years ago and are now facing a different standard.
This guide is built for that exact situation. It explains va disability gerd acid reflux in plain language, shows how the 2024 rating changes affect claims, and gives practical symptom-management ideas you can use while your claim moves forward. If you are also trying to improve day-to-day comfort, some veterans find it helpful to keep a simple symptom journal alongside visual resources like this digestive wellness image library: https://healthygutreview.com/wp-content/uploads/2026/04/culturelle-digestive-health-probiotic-reviews-probiotic-gut.jpg
{kind=link}
Your Guide to VA Disability for GERD and Acid Reflux
A lot of veterans come into this process thinking acid reflux is “too common” or “not serious enough” to rate. That belief stops good claims before they even start. The VA does recognize GERD, and the details matter.
The first thing to know is simple. A diagnosis alone is not the whole claim. The VA wants to know how your condition connects to service and how severe it is now.
For many veterans, the hard part is not proving they have reflux. The hard part is translating years of symptoms into the kind of evidence the VA uses. Burning after meals, choking episodes at night, trouble swallowing, medication changes, and missed sleep all need to be documented clearly.
Key takeaway: Treat your GERD claim like a medical story with three parts. When it started, why it connects to service, and how it affects you now.
The good news is that the rules are more specific than they used to be. That can help if your records show the right findings. It can also hurt if your symptoms are real but poorly documented. That is why strong records and clear language matter so much.
Establishing Service Connection for GERD
Service connection is the foundation of your claim. If the VA does not connect your GERD to service, the rating question never really gets off the ground.
GERD is common in the veteran community. 25.52% of veterans treated within the VA system have been diagnosed with GERD, and veterans can pursue claims as a stand-alone condition or as secondary to disabilities like PTSD, anxiety, or respiratory conditions, according to Hill & Ponton’s discussion of service connection for GERD.
Direct service connection
This path fits veterans whose reflux symptoms began during active duty or can be traced to something that happened there.
Think of direct service connection as a straight line. You had symptoms, treatment, complaints, or an event in service, and you still deal with GERD now.
Useful evidence can include:
- Service treatment records: Notes about heartburn, reflux, chest burning, throat irritation, or repeated sick-call visits.
- Post-service continuity: Records showing the symptoms kept going after discharge.
- Personal statements: A timeline in your own words that connects the in-service symptoms to the diagnosis you have now.
If you were never formally diagnosed during service, do not assume the claim is dead. Many veterans were treated for symptoms without the chart ever using the word GERD.
Secondary service connection
This is one of the strongest paths for many veterans.
Secondary service connection means another service-connected disability, or treatment for it, caused or worsened your GERD. A common example is a veteran with a service-connected orthopedic injury who uses NSAIDs for pain and develops worsening reflux. Another example is a veteran with service-connected PTSD whose stress symptoms and treatment history line up with chronic reflux.
Here is the practical test. Ask yourself whether your GERD got worse after another service-connected problem began, after medication changes, or during periods when that primary condition flared.
Aggravation
Aggravation applies when you had reflux issues before service, but military service made them permanently worse.
Veterans often get tripped up on this point. Temporary flare-ups are not the same as aggravation. The VA is looking for evidence that the baseline condition became more severe over time because of service demands, exposures, treatment, or related conditions.
How to decide which path fits
Use the path your records support best.
| Path | What it means in plain English | Best supporting evidence |
|---|---|---|
| Direct | GERD started in service or from an in-service event | In-service records, early post-service treatment, symptom timeline |
| Secondary | Another service-connected condition or its treatment caused GERD | Primary rating, medication history, medical opinion linking the two |
| Aggravation | A preexisting reflux condition became permanently worse | Records showing baseline symptoms before service and worse symptoms after |
Practical tip: Do not force a direct claim if the stronger evidence points to PTSD, anxiety, respiratory disease, or medication side effects. The strongest theory is the one your records can prove.
Understanding the VA Rating Schedule for GERD
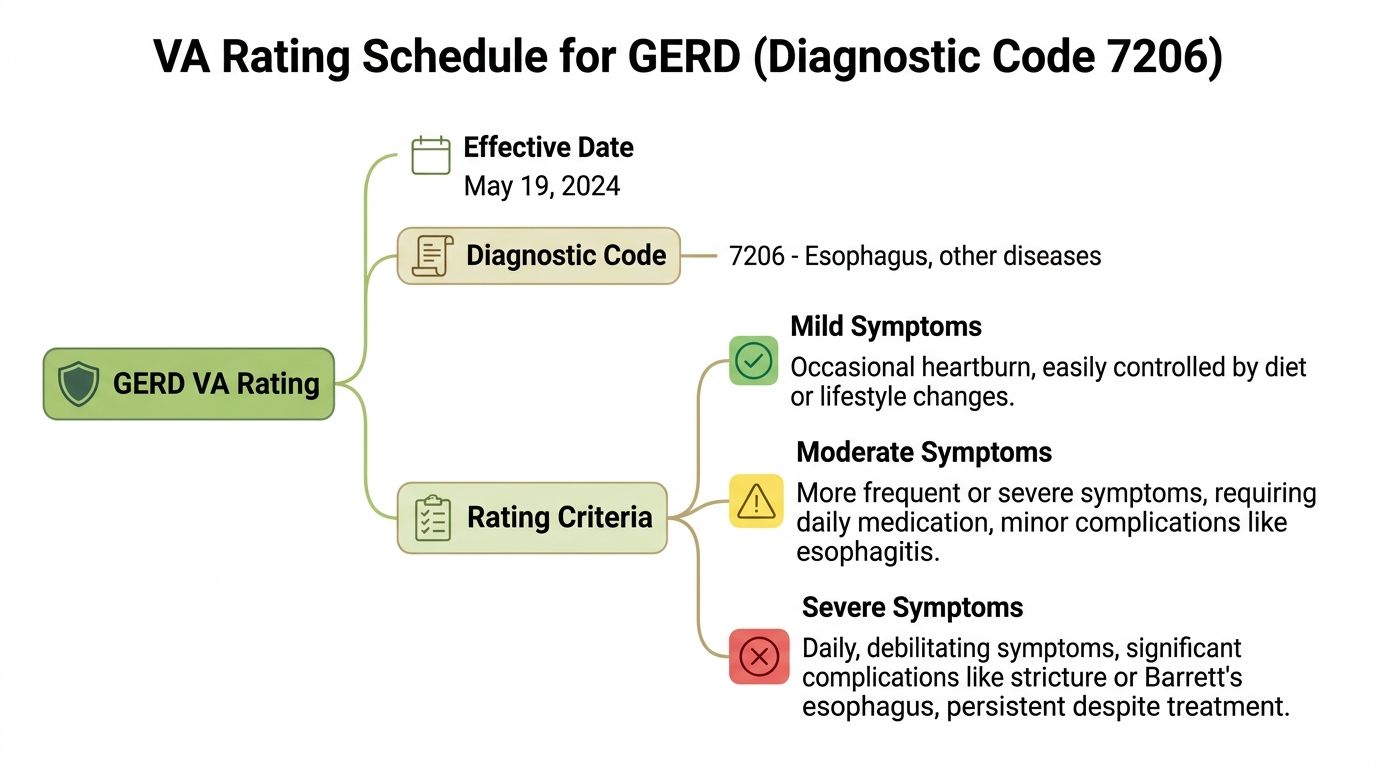
The biggest recent change is that the VA now rates GERD under Diagnostic Code 7206, effective May 19, 2024, with ratings of 0%, 10%, 30%, 50%, or 80%. The new criteria focus on esophageal strictures, dysphagia, and related complications rather than the older hiatal-hernia-style approach, as outlined in this overview of the updated GERD VA rating criteria.
What the new terms mean
The rating language sounds technical, but the ideas are not impossible.
Dysphagia means trouble swallowing.
Esophageal stricture means narrowing in the esophagus.
Dilatation means a procedure to widen that narrowing.
Stent placement means a device is placed to help keep the area open.
That matters because the newer schedule is less about general discomfort alone and more about objective evidence showing that reflux has damaged swallowing function or created serious complications.
VA disability ratings for GERD under DC 7206
| Rating % | Key criteria and symptoms |
|---|---|
| 0% | Documented history with no daily symptoms and no daily medication requirement |
| 10% | Esophageal stricture history requiring daily medications to control dysphagia, otherwise asymptomatic |
| 30% | Recurrent stricture causing dysphagia, requiring dilatation no more than two times per year |
| 50% | Recurrent or refractory strictures causing dysphagia and requiring dilatation three or more times per year, dilatation with steroids once yearly, or esophageal stent placement |
| 80% | Recurrent or refractory strictures causing dysphagia with complications such as aspiration, undernutrition, or substantial weight loss requiring surgical correction or PEG tube placement |
How to think about each rating
A 0% rating still matters. It means the VA recognizes service connection, even if your current symptoms do not qualify for monthly compensation. That can help later if the condition worsens.
A 10% rating usually fits veterans who need daily medication to control swallowing-related symptoms tied to the condition. This is the minimum level needed for compensation.
A 30% rating means the records show recurring narrowing severe enough to require periodic dilatation, but not more than two times per year.
A 50% rating reflects a much more disruptive pattern. The VA is looking for recurrent or refractory strictures with more frequent intervention, steroid-assisted dilatation, or stent placement.
An 80% rating is reserved for severe cases involving major complications. The verified criteria include aspiration or substantial weight loss requiring surgery or PEG tube placement.
Where veterans get confused
The confusion usually comes from older advice. Under the old system, many GERD claims were rated by analogy to hiatal hernia rules. Some veterans still have older claims or older ratings that were built under that approach.
If you were rated before the change, the practical question is not “Which system is newer?” The practical question is “Which system is more favorable to my evidence?”
Important point: The new schedule rewards strong objective findings. If your medical record talks in detail about swallowing problems, procedures, and complications, that becomes much more important now.
Building Your Evidence File for a Strong Claim
A solid GERD claim is built with records, not guesses. You want the VA examiner and rater to see a clean paper trail that matches your symptoms.
One useful overview of claim evidence notes that endoscopy (EGD), 24-hour pH monitoring, and manometry can support a GERD claim, and that pharmacy records showing escalating PPI use can help answer “medication-controlled” denials. It also notes that nexus letters linking service stressors such as PTSD to GERD can help secondary claims, as described in this guide on GERD-related VA claim evidence.
Start with the medical core
Think of your file in layers. The first layer is objective testing and treatment records.
Prioritize these documents:
- Endoscopy reports: Especially if they mention stricture, inflammation, or other visible findings.
- 24-hour pH monitoring: Helpful when reflux needs objective confirmation.
- Manometry results: Useful if swallowing problems or motility issues are part of the picture.
- Procedure records: Dilatations, stent placement, or surgical recommendations.
- Pharmacy history: Refill records, dose changes, medication failures, and step-ups in treatment.
A veteran who says, “I have bad reflux,” gives the VA a symptom. A veteran who submits endoscopy findings, refill history, and procedure notes gives the VA a case.
Here is a helpful video overview before you organize your file:
Do not overlook the nexus letter
The nexus letter is often the missing link.
This is a medical opinion from a qualified clinician explaining why your current GERD is at least as likely as not related to service, a service-connected condition, or treatment for that condition. The strongest letters do more than state a conclusion. They explain the medical reasoning.
Ask the clinician to address:
- Your diagnosis
- The service event or primary service-connected condition
- Why the connection makes medical sense
- Whether the condition caused or aggravated your GERD
For secondary claims, this can be especially important when PTSD, anxiety, chronic pain treatment, or respiratory conditions are part of the story.
Add lay evidence that fills the gaps
Medical tests matter, but daily life evidence helps the VA understand severity.
Good lay evidence can come from:
- Your own statement: Describe sleep disruption, food avoidance, choking, missed work, or pain after meals.
- Spouse or partner statement: They may have seen nighttime reflux, coughing, vomiting, or strict eating habits.
- Buddy statements: Helpful if symptoms were visible during service.
- Coworker observations: Useful when GERD affects attendance, meal breaks, or performance.
Practical tip: Write your statement like a timeline, not a rant. Explain when symptoms started, how often they happen, what treatment you use, and what still happens despite treatment.
A simple evidence checklist
| Evidence type | Why it helps |
|---|---|
| Diagnosis and treatment notes | Shows the condition is current and ongoing |
| EGD, pH monitoring, manometry | Provides objective support |
| Pharmacy records | Shows persistence and treatment intensity |
| Nexus letter | Connects GERD to service or a primary disability |
| Lay statements | Shows real-world impact on sleep, meals, and work |
7 Strategies and Products to Manage GERD Symptoms
Medication helps many veterans, but it does not solve everything. A practical gap in many va disability gerd acid reflux guides is daily symptom management. One source in the background material notes that 40% to 60% of GERD patients report incomplete relief from medications alone, and it highlights diet changes and targeted probiotics as useful complementary strategies in this discussion of practical GERD management gaps.
Below are seven supportive strategies paired with Amazon products veterans often consider. These are not cures, and they are not a substitute for medical care. They are tools that may help you manage symptoms while also giving you a clearer picture of what triggers your reflux.
1. Sleep on an incline
Product: MedCline Acid Reflux Relief System
Sleeping flat can make nighttime reflux harder to control. An incline system may reduce the need to stack random pillows that slide around by midnight.
Pros
- Built for reflux support: Designed specifically for upper-body elevation.
- Can improve sleep positioning: Many users prefer it to loose pillows.
- Useful for symptom tracking: If nighttime symptoms ease or persist, that is helpful information for your records.
Cons
- Bulky setup: It takes space.
- Adjustment period: Side sleepers and restless sleepers may need time to adapt.
- Higher cost than a basic wedge pillow
Bottom line: This is one of the strongest product options for veterans whose worst reflux hits overnight.
2. Use a simpler wedge pillow if you want a lower-cost option
Product: Lunix Bed Wedge Pillow
Not everyone wants a full reflux sleep system. A wedge pillow is the simpler version.
Pros
- More affordable entry point
- Easy to try without replacing your mattress
- Can help keep your upper body elevated after meals or before sleep
Cons
- Fit varies by sleeper
- Can slide or compress over time
- Some users still need additional pillow support for neck comfort
A wedge is often the practical choice if you want to test elevation before spending more.
3. Track trigger foods and simplify meal planning
Product: The Acid Watcher Diet book
Food triggers are highly individual. One veteran may react to tomato sauce and coffee. Another may struggle more with late meals, fried food, or large portions.
A structured meal guide can make the process less random. If you want recipe ideas and food-planning support, some readers also browse resources like this reflux-focused cookbook collection: https://healthygutreview.com/wp-content/uploads/2026/04/acid-reflux-gerd-diet-recipes-recipe-books.jpg
{kind=link}
Pros
- Helps create consistency: That matters when you are trying to identify patterns.
- Useful for a symptom journal: Meals are easier to log when you follow a structure.
- Supports non-medication management
Cons
- Diet books are only useful if you follow them
- Some recipes may not match your preferences
- Elimination-style eating can feel restrictive at first
Tip: Keep a food and symptom log for a few weeks. Record meals, timing, symptoms, sleep disruption, and medication use. That log can help both your health routine and your claim narrative.
4. Try a probiotic with digestive support in mind
Product: Culturelle Digestive Daily Probiotic
Some veterans dealing with GERD also deal with bloating, irregular digestion, or gut disruption after long periods of medication use. A probiotic will not “fix” structural reflux, but it may support overall digestive comfort for some people.
Pros
- Simple once-daily format
- Widely available on Amazon
- May be a practical add-on for veterans who also have bloating or digestive imbalance
Cons
- Responses vary from person to person
- Not a replacement for GERD treatment
- Some users need time to assess tolerance
This is a support tool, not a primary GERD treatment. Think of it as part of a broader gut-health plan.
5. Consider DGL licorice for soothing support
Product: Natural Factors DGL Licorice Chewable Tablets
Some people use DGL licorice before meals for upper-digestive soothing support.
Pros
- Chewable and easy to use
- Popular among people looking for non-prescription digestive support
- Can fit into a meal-based routine
Cons
- Taste is not for everyone
- Not appropriate for every veteran
- Should be cleared with your clinician if you take other medications or have health concerns
This can be a reasonable product to discuss with your healthcare team if you want a non-prescription support option.
6. Reduce oversized late meals
Product: Bentgo Prep meal prep containers
This is not glamorous, but it helps. Many reflux flare-ups come from meal timing and portion size rather than one dramatic trigger food.
Meal prep containers support smaller, earlier, more predictable meals.
Pros
- Makes portion control easier
- Helps avoid giant end-of-day meals
- Useful for work shifts and appointments
Cons
- Requires planning
- Only helps if you prep meals
- Storage space can become a hassle
For many veterans, this is one of the most realistic reflux strategies because it changes daily habits instead of adding another supplement.
7. Raise the head of the bed more securely
Product: Utopia Bedding Adjustable Bed Risers
If a wedge pillow keeps shifting, bed risers may give you a more stable incline.
Pros
- Simple setup
- Can work with your current mattress
- May help people who dislike sleeping on foam wedges
Cons
- Not ideal for every bed frame
- Can feel awkward at first
- You need to install them carefully for stability
Which product is the winner
If I had to choose one winning product for the broadest group of veterans with nighttime symptoms, I would pick the MedCline Acid Reflux Relief System.
Why that one? Because nighttime reflux can wreck sleep, and poor sleep makes everything harder. It affects energy, stress tolerance, meal choices, and how clearly you can describe your symptoms at appointments. A reliable incline setup addresses one of the most common and disruptive parts of GERD.
The best value option is the Lunix Bed Wedge Pillow. The best low-tech habit tool is meal prep containers because they support earlier, smaller meals in a practical way.
A note on quotes and reviews. Product reviews on Amazon change constantly, and I do not want to invent language or ratings. When you compare these items, look for reviews that mention sleep comfort, material quality, odor, stability, ease of cleaning, and whether users noticed less nighttime reflux.
Navigating Your C&P Exam and Filing Your Claim
The C&P exam is where many veterans accidentally weaken their own case. They minimize symptoms, forget key details, or talk in general terms that do not match the rating language.
How to talk about symptoms clearly
Do not say, “I have reflux sometimes.”
Say what happens. Explain whether you wake up choking, avoid certain foods, need daily medication, have trouble swallowing, or have had testing or procedures. Explain what happens on your worst days, not just your best days.
Good symptom language sounds like this:
- Frequency: “This happens most days.”
- Function: “I avoid certain meals and cannot lie down comfortably after eating.”
- Impact: “It disrupts my sleep and leaves me tired at work.”
- Treatment history: “I still have symptoms even with medication and diet changes.”
What not to do at the exam
A few common mistakes cause trouble fast.
- Do not downplay symptoms: Veterans often do this out of habit.
- Do not exaggerate: If your records and your exam story do not match, credibility suffers.
- Do not forget daily impact: Sleep, meals, swallowing, work, and medication side effects matter.
- Do not assume the examiner read everything: Bring your memory, not just your file.
Exam tip: Before the appointment, write down your top five symptoms, your current medications, recent testing, and two examples of how GERD affects daily life. Read that list in the parking lot if needed.
Filing the claim
For many initial claims or increase claims, veterans use VA Form 21-526EZ. You can generally file online, by mail, or with the help of a representative such as a VSO, accredited agent, or attorney.
Keep the filing package organized:
| Filing item | What to include |
|---|---|
| Claim form | Correct form and basic condition details |
| Medical records | Diagnosis, testing, treatment, procedures |
| Personal statement | Symptom history and daily impact |
| Nexus evidence | Especially important for secondary claims |
| Supporting statements | Family, buddy, or coworker observations if useful |
If the VA denies the claim
A denial is not always the end of the road. Sometimes the problem is not the condition itself. It is the missing link, weak wording, or incomplete evidence.
Read the decision carefully. Look for the exact reason. Was service connection denied? Was the rating too low? Did the VA say symptoms were controlled by medication or that there was not enough objective evidence? Your next move depends on that answer.
Taking Control of Your Health and Your Claim
A strong GERD claim comes down to three things. A clear service connection theory, evidence that matches the rating criteria, and a believable description of daily impact.
That process takes patience. It also helps to work on both tracks at once. Build the claim carefully, and manage the condition consistently.
If reflux is affecting your sleep, meals, and daily routine, start documenting that now. Keep records of symptoms, treatment changes, and what happens despite your best efforts. That kind of consistency helps your health and strengthens your file.
The bigger point is this. You are not stuck waiting for the VA to define your experience for you. You can organize the evidence, prepare for the exam, and make your case in a way that reflects what your life looks like. Some veterans also stay motivated by building healthier meal habits with supportive resources like this anti-inflammatory foods book collection: https://healthygutreview.com/wp-content/uploads/2026/04/books-on-anti-inflammatory-foods-healthy-foods.jpg
{kind=link}
Frequently Asked Questions About VA Disability for GERD
Can I get VA disability for GERD if I was diagnosed after service
Yes, sometimes. A post-service diagnosis can still work if the evidence shows symptoms began in service, continued after discharge, or were caused or aggravated by another service-connected condition.
Is GERD a stand-alone claim or usually secondary
It can be either one. Some veterans claim it directly. Others have a stronger case claiming it as secondary to PTSD, anxiety, respiratory issues, or medication use related to another service-connected disability.
Do I need a current diagnosis
Yes. A current diagnosis is the starting point. Without it, the VA usually has no condition to rate.
What evidence helps the most
The best evidence is usually a combination of medical records, objective testing, treatment history, and a strong nexus opinion when service connection is not obvious. Personal statements also help show how symptoms affect sleep, eating, and work.
Can I get compensation with a 0 percent rating
No monthly compensation comes with a 0% rating, but it still establishes service connection. That can matter later if the condition worsens or leads to secondary problems.
What should I bring to a C&P exam
Bring a clear memory of your symptoms, medication list, testing history, and examples of how GERD affects your daily life. If you freeze up during appointments, make brief notes ahead of time.
Can lifestyle changes hurt my claim
No. Trying to manage symptoms does not weaken your case. In many situations, it helps show that the condition is persistent and requires ongoing effort to control.
If you want more practical digestive wellness guidance alongside evidence-based product reviews, visit Healthy Gut Review. It is a useful place to compare gut health tools, learn food strategies, and build a symptom-management routine that supports your day-to-day life while you work through the VA process.