

Dinner is over. You sit down on the couch, and within minutes you feel that familiar burn rising from your upper stomach into your chest. Maybe there is a sour taste in your mouth. Maybe it happens after pizza, takeout, coffee, or a late-night snack. You wonder if this is just heartburn, or if something more serious is starting.
That confusion is common. People often use acid reflux, heartburn, and GERD as if they mean the same thing. They do not. Heartburn is a symptom. Acid reflux is the process causing that symptom. GERD is a chronic disease state that develops when reflux happens often enough, long enough, or severely enough to need medical attention.
If you have been searching what is the difference between gerd and acid reflux, the short answer is this: acid reflux is occasional backflow of stomach contents into the esophagus, while GERD is ongoing reflux that becomes a health problem. The details matter, because the right response for a once-in-a-while episode is different from the right response for symptoms that keep returning.
Is It Just Heartburn or Something More Serious
A lot of people first notice reflux in an ordinary moment. A heavy dinner. A spicy lunch. Bending over to unload groceries. Lying flat too soon after eating. Then comes the burning feeling, throat irritation, or sour liquid creeping upward.
For some people, it happens once in a while and then disappears for weeks. For others, it starts showing up so often that they plan meals around it, sleep propped up on pillows, or keep antacids in every bag and nightstand drawer.
That difference matters.
One patient might tell me, “I only feel it after a huge restaurant meal.” Another says, “I wake up with it, I get it at work, and I avoid eating before meetings because I know it will flare.” Those are not the same clinical picture, even if both people use the word heartburn.
Why the terms get mixed up
People usually describe what they feel, not what the diagnosis is.
- Heartburn is the burning sensation.
- Acid reflux is the backward flow of stomach acid.
- GERD is the ongoing condition where reflux becomes frequent or damaging.
That is why one person can have heartburn without having GERD, and another can have GERD with symptoms beyond classic burning, such as cough, hoarseness, or regurgitation.
What readers usually worry about
Many people ask a practical question, not a technical one.
They want to know:
- Is this normal: Did I just eat something that triggered a one-off episode?
- Is this becoming chronic: Am I crossing into something that needs a doctor?
- What can I do tonight: Should I change meals, timing, posture, or medication use?
- Could my gut be involved: If I also deal with bloating, gas, or irregular digestion, is reflux part of a bigger picture?
Even meal pattern changes, like shifting toward lighter anti-inflammatory meals, can affect symptom load for some people. A visual example of that kind of eating pattern appears in this anti-inflammatory meal box image.
{kind=link}
If your symptoms are occasional, the conversation is usually about triggers. If your symptoms are frequent, the conversation shifts to tissue irritation, complications, and proper diagnosis.
Understanding Acid Reflux The Occasional Annoyance
Acid reflux is the backward flow of stomach contents into the esophagus, the tube that carries food from your mouth to your stomach. The lower esophageal sphincter, or LES, is a muscular ring that acts as a valve. It opens to let food into the stomach and then closes to keep stomach contents where they belong. If it relaxes at the wrong time, acid and partially digested food can rise upward and irritate the esophagus.

What occasional reflux feels like
An occasional episode often shows up after a large meal, a late dinner, or lying down too soon after eating. You may notice:
- Burning in the chest: Often after meals or when reclined
- A sour or bitter taste: Stomach contents reaching the throat or mouth
- Mild throat irritation: More noticeable after regurgitation
- Bloating or pressure: Fullness in the upper abdomen that seems to push upward
One point that gets missed is that reflux does not always start with “too much acid.” Sometimes it starts with pressure. If your stomach is overly full, digestion is slow, or gas builds up from fermentation in the upper gut, that extra pressure can make reflux more likely.
Why occasional reflux happens
The stomach is designed to handle acid. The esophagus is not. Even a brief splash upward can irritate the lining and cause that familiar burning sensation.
For some people, the trigger is mostly mechanical. A heavy meal stretches the stomach. Lying flat removes gravity’s help. Tight clothing, constipation, or frequent bloating can also increase upward pressure.
For others, the pattern points to digestion happening less smoothly than it should. If reflux tends to come with belching, early fullness, abdominal swelling, or symptoms after healthy foods that should be easy to tolerate, it may be worth asking whether gut imbalance is part of the picture. Conditions such as SIBO can increase gas production in the small intestine. More gas can mean more pressure pushing upward against the LES.
Common triggers
Occasional reflux often has a clear setup, even if the exact food varies from person to person.
Common examples include:
- Large meals: A fuller stomach creates more pressure
- Eating close to bedtime: Food is still in the stomach when you lie down
- Spicy, rich, or high-fat meals: These can worsen symptoms in sensitive people
- Coffee or alcohol: Some people notice more reflux after either one
- Bloating and excess gas: Pressure from fermentation can make reflux easier to trigger
This is one reason a food and symptom log can help. You are not only looking for acidic foods. You are looking for patterns such as volume, timing, bloating, belching, and whether certain carbohydrates seem to trigger both gas and reflux.
What helps when it is occasional
Start simple.
- Eat smaller meals and chew slowly.
- Stay upright for a few hours after eating.
- Finish dinner earlier if nighttime symptoms are the problem.
- Track bloating, belching, and bowel changes along with reflux symptoms.
- Use over-the-counter relief sparingly for isolated episodes, not as a daily routine without guidance.
If you also deal with frequent bloating or suspected SIBO, gut-focused support may matter as much as avoiding trigger foods. In practice, that can mean reviewing fermentable foods, discussing whether a probiotic is appropriate for your symptom pattern, and using supplements carefully. Some people do well with targeted probiotics, while others with active SIBO feel worse with the wrong product. Ginger, alginate formulas, and digestive support strategies may help some patients, but they work best when matched to the reason reflux is happening.
If reflux is occasional and tied to a clear trigger, it often improves with meal timing, portion changes, and better management of bloating and gut imbalance.
Defining GERD When Reflux Becomes a Chronic Disease
You finish dinner, go to bed, and wake up at 2 a.m. with burning in your chest and a sour taste in your throat. A week later, it happens again. Then you start keeping antacids by the bed, skipping foods you enjoy, and wondering whether this is still ordinary reflux or something that needs medical care.
That shift in pattern is what matters.
GERD stands for gastroesophageal reflux disease. Clinicians use this term when reflux stops being occasional and starts showing up often enough, long enough, or strongly enough to affect the esophagus and daily life. The stomach is built to handle acid. The esophagus is not, so repeated backflow can irritate its lining much like repeated skin friction can turn a small rub into a raw spot.
When does reflux cross into GERD?
A practical cutoff many clinicians use is symptoms at least twice a week for several weeks, especially if they disturb sleep, eating, or normal activities.
Frequency is only part of the picture, though. GERD can also mean reflux that keeps returning even when you try the usual fixes, or reflux that comes with signs of irritation outside the classic burning feeling. Some people notice regurgitation, a chronic cough, hoarseness, throat clearing, or a feeling that food is slow to go down.
What makes GERD different in the body
With GERD, the problem is repeated exposure. Acid, and sometimes other stomach contents, wash upward often enough that the esophagus does not get a chance to recover fully between episodes.
Over time, that can lead to:
- Frequent heartburn
- Regurgitation of food or sour liquid
- Pain or pressure in the chest
- Trouble swallowing
- Hoarseness, throat irritation, or cough
- Nighttime symptoms that interrupt sleep
Many patients are surprised by the throat and sleep symptoms. Reflux does not always stay in the lower chest. If stomach contents reach higher, the throat and voice box can become irritated too.
Why some cases become chronic
GERD is often described as a valve problem, and that is part of the story. The lower esophageal sphincter works like a lid between the esophagus and stomach. If it relaxes too often or does not close well, reflux happens more easily.
But chronic reflux is not always just about acid strength or one weak muscle. Pressure inside the abdomen, slow stomach emptying, bloating, constipation, and bacterial overgrowth can all make reflux harder to control. Here, the gut microbiome perspective matters.
If food is fermenting higher in the digestive tract, as can happen with SIBO, extra gas can build pressure in the stomach and upper small intestine. More pressure can push contents upward, especially after meals or when lying down. That does not mean every person with GERD has SIBO, but it helps explain why some people keep having reflux along with bloating, belching, and fullness even when they are avoiding obvious trigger foods.
Why repeated reflux deserves attention
Chronic reflux can inflame the esophagus and make symptoms more stubborn over time. It can also change how you eat, sleep, exercise, and socialize. Patients often tell me the turning point was not the burn itself. It was planning the day around it.
That is also the stage where self-treatment has limits. If you need frequent antacids, rely on acid reducers week after week, or keep getting symptoms despite being careful with meals, it is time for a proper evaluation.
A simple self-check
Ask yourself:
- Do symptoms show up multiple times most weeks?
- Have they been going on for several weeks or longer?
- Do they wake you from sleep?
- Are you using over-the-counter relief regularly?
- Do you also have bloating, belching, early fullness, or bowel changes that suggest a gut imbalance may be part of the picture?
- Have you noticed swallowing trouble, chronic cough, hoarseness, or food coming back up?
If several of those fit, you may be dealing with GERD rather than isolated acid reflux.
GERD means reflux has become a recurring condition, not a one-off event. The pattern matters, the impact matters, and in some people the deeper issue includes pressure from bloating, microbiome disruption, or SIBO alongside acid exposure.
Acid Reflux vs GERD A Side-by-Side Comparison
The clearest way to answer what is the difference between gerd and acid reflux is to compare them directly. They share the same basic mechanism, but they differ in pattern, impact, and risk.
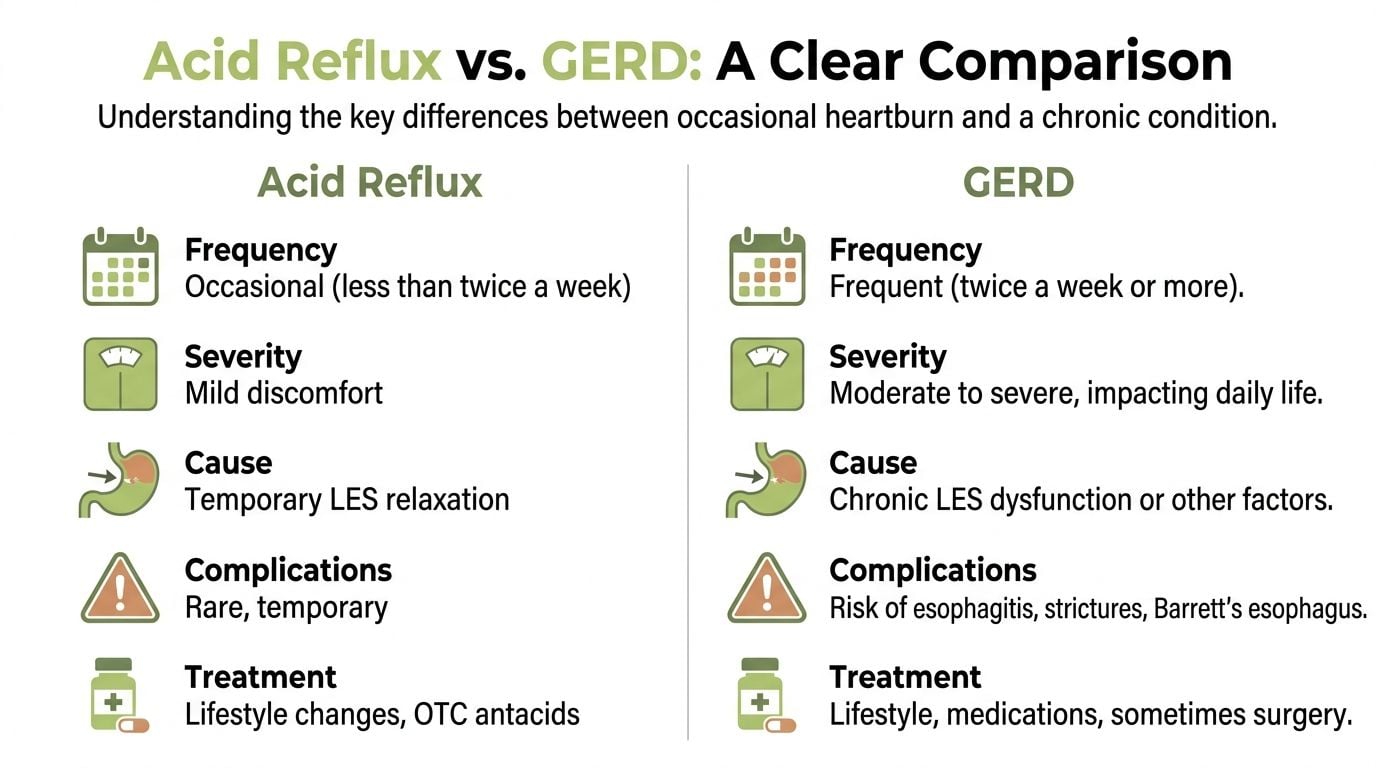
Key Differences Between Acid Reflux and GERD
| Criterion | Acid Reflux (Occasional) | GERD (Chronic Disease) |
|---|---|---|
| Frequency | Happens once in a while, often after a trigger | Happens repeatedly, usually at least twice a week for several weeks |
| Pattern | Episodic | Ongoing or recurrent |
| Cause | Temporary LES relaxation | Persistent reflux pattern with ongoing LES dysfunction or related factors |
| Symptoms | Heartburn, sour taste, mild regurgitation | Heartburn plus regurgitation, nighttime symptoms, swallowing issues, cough, throat irritation |
| Impact on daily life | Usually limited | Can affect meals, sleep, work, and comfort |
| Tissue damage risk | Usually low when episodes are occasional | Higher if untreated because acid exposure keeps recurring |
| Typical response | Trigger control and occasional OTC relief | Medical evaluation, structured treatment, and monitoring may be needed |
Frequency is the biggest dividing line
If symptoms happen only now and then, especially after a recognizable trigger, that leans toward acid reflux.
If symptoms happen over and over, week after week, that leans toward GERD. Frequency changes the clinical meaning of the symptom.
Severity is not only about pain
A person can have moderate discomfort but still have GERD if the symptoms are chronic. Another person can have one miserable night after overeating and still not have GERD.
Look at the whole pattern:
- Occasional reflux: uncomfortable, but limited
- GERD: recurring enough to disrupt normal living
The symptom list also widens with GERD
Acid reflux often stays in the “burning and sour taste” category.
GERD can look broader. People may report:
- coughing that will not quit
- hoarseness in the morning
- a sensation of food sticking
- bad breath linked to regurgitation
- chest symptoms that feel alarming
That broader symptom picture is one reason GERD can be missed.
Long-term risk is where the distinction matters most
With occasional reflux, the goal is usually symptom control.
With GERD, the goal is symptom control and protection of the esophagus. Chronic exposure raises the chance of inflammation and structural complications. That is why persistent symptoms deserve proper diagnosis instead of endless self-treatment.
A quick real-life example
Consider these two scenarios.
Person A: Gets burning after a large, spicy restaurant meal, takes an antacid, and feels fine the next day. No symptoms the rest of the week.
Person B: Feels burning several times a week, sleeps upright to cope, coughs at night, and avoids certain meals out of fear.
Person A sounds like occasional acid reflux. Person B sounds much more like GERD.
How to think about it
Use this rule of thumb:
- Occasional and trigger-based usually points to acid reflux.
- Frequent, recurring, or disruptive points to GERD.
That does not replace a diagnosis, but it helps you decide when home strategies may be enough and when it is time to involve a clinician.
The same symptom, heartburn, can belong to two very different situations. The deciding factors are how often it happens, how much it affects life, and whether the esophagus may be getting injured.
Red Flag Symptoms That Signal More Than Just Reflux
You wake up with burning in your chest again, reach for the same antacid, and tell yourself it is probably the meal from last night. That is a common choice. It becomes a risky one when the symptom pattern changes.
Reflux is often manageable at home. Bleeding, trouble swallowing, repeated vomiting, and chest pain that feels different need medical attention because they can point to irritation, narrowing, ulcers, or a problem outside the digestive tract.

Symptoms that deserve prompt medical attention
Contact your clinician promptly, or seek urgent care based on severity, if you notice:
- Difficulty swallowing: Food feels stuck or slow to go down
- Pain with swallowing: This can signal significant irritation or an ulcer
- Vomiting blood or material that looks like coffee grounds: This needs urgent evaluation
- Black stools: This can suggest gastrointestinal bleeding
- Chest pain: Especially if it is severe, new, or hard to separate from a heart problem
- Ongoing vomiting: This can lead to dehydration and may signal a blockage or severe inflammation
- Unexplained weight loss or loss of appetite: These symptoms deserve a medical review, even if reflux seems like the obvious cause
Why swallowing symptoms matter
Swallowing should feel smooth and automatic, like food sliding down a well-lubricated tube. When that tube becomes inflamed or narrowed, the process changes. Patients often describe it as food hesitating, hanging up, or moving down slowly.
That pattern can happen with esophageal inflammation, scarring, or a stricture. It should not be managed with trial-and-error supplements or repeated antacids alone.
Cough, throat symptoms, and dental changes can point to a broader problem
Some warning signs show up far from the lower chest. Stomach contents can reach the throat and mouth, irritating tissues that are not built to handle acid and enzymes.
You might notice:
- morning hoarseness
- frequent throat clearing
- chronic dry cough
- wheezing that flares after meals or at night
- enamel wear your dentist mentions
- sour taste or regurgitation during sleep
Here is a short explainer that helps connect those dots:
A gut health clue many people miss
If reflux comes with bloating, belching, early fullness, or pressure after eating, I start thinking beyond acid alone. In some patients, poor motility or small intestinal bacterial overgrowth, often called SIBO, can increase gas and abdominal pressure. That pressure works like air building up in an overfilled container. It can push stomach contents upward and make reflux harder to control.
That does not mean every person with GERD has SIBO. It does mean recurring reflux with a lot of bloating deserves a fuller evaluation instead of months of guessing.
For practical food ideas that are gentler on reflux while you sort out triggers, a reflux-friendly diet and recipe guide can help you plan meals with less trial and error.
{kind=link}
Be careful with self-treatment if alarm signs are present
Some probiotics, digestive products, and herbal supplements can support gut health in the right setting, especially when bloating and microbiome imbalance are part of the picture. They are not the first answer for bleeding, progressive swallowing trouble, severe chest pain, or persistent vomiting.
Those symptoms need diagnosis first.
Chest pain needs caution
Chest pain from reflux can feel burning, squeezing, or sharp. Heart-related pain can feel similar. Seek emergency help right away if chest pain comes with shortness of breath, sweating, faintness, nausea, or pain spreading to the arm, jaw, shoulder, or back.
If symptoms are escalating, changing, or starting to affect swallowing, breathing, or eating, stop treating it like routine heartburn and get medical care.
How Doctors Diagnose and Treat GERD
You have had heartburn on and off for months. Now it is showing up at night, you are buying remedies more often, and you are starting to wonder whether this is still “just reflux” or something that needs a proper workup. That is usually the point where a clinic visit becomes useful.
A doctor is trying to answer a few practical questions. Are your symptoms caused by reflux? Has the esophagus been irritated or injured? Is there another problem mixed in, such as trouble with stomach emptying, a hiatal hernia, or bloating patterns that raise concern for gut imbalance or SIBO?
How diagnosis usually starts
The first step is often a careful history, not a procedure.
Your clinician will ask what the symptoms feel like, how often they happen, whether they wake you from sleep, whether food seems to trigger them, and whether you feel acid coming up into the throat or mouth. They will also ask about belching, bloating, early fullness, nausea, bowel changes, and medicines you take. Those details matter because reflux can be driven by more than acid alone. In some people, excess gas and pressure in the upper gut make the valve between the esophagus and stomach more likely to open.
A basic exam may follow, but many reflux cases are diagnosed from the symptom pattern first.
Tests doctors may use
Not everyone needs testing right away. The choice depends on your age, symptom pattern, response to treatment, and whether warning signs are present.
Common options include:
- Upper endoscopy: A thin camera examines the esophagus, stomach, and first part of the small intestine. This helps check for inflammation, narrowing, ulcers, or tissue changes.
- Ambulatory pH monitoring: A small device measures how much acid reaches the esophagus over a day or more. This is especially helpful when the diagnosis is unclear or symptoms continue despite treatment.
- Esophageal manometry: This checks how the esophagus squeezes and how the lower esophageal sphincter functions. It is often used before certain procedures or when swallowing symptoms are part of the picture.
- Targeted testing for related issues: If bloating, distention, or excessive belching stand out, a clinician may also consider whether constipation, delayed stomach emptying, food intolerance, or SIBO is adding pressure and worsening reflux.
That last point is often missed. Some people are treated for acid for months when the bigger driver is pressure from fermentation and gas lower in the digestive tract.
What treatment usually involves
GERD treatment usually happens in layers. The goal is not only to calm symptoms, but also to reduce repeated irritation and choose a plan you can realistically follow.
Food habits and body positioning
Simple changes still help many patients, especially when symptoms are linked to meal size and timing.
Doctors often recommend smaller meals, less late-night eating, and staying upright after food. Tight waistbands, heavy bending after meals, and large high-fat meals can all increase upward pressure. If you need practical meal ideas while sorting out your triggers, this reflux-friendly GERD diet recipe guide gives a helpful example of the kind of planning many people use.
Over-the-counter medicines
For milder symptoms, short-term nonprescription treatment may be reasonable.
- Antacids work quickly and can help with occasional breakthrough symptoms.
- H2 blockers last longer and may help when symptoms happen more regularly, including at night for some patients.
These options can be useful, but frequent reliance on them is a sign to get clearer answers instead of continuing to guess.
Prescription treatment
If symptoms are frequent, the esophagus looks inflamed, or over-the-counter treatment is not enough, clinicians often prescribe stronger acid suppression, usually with an H2 blocker or a proton pump inhibitor.
These medicines lower acid exposure so the esophagus has a chance to heal. Timing matters. Many people get poor results because they take the medicine at the wrong time of day or stop too early. A clinician can also help decide whether your symptoms are acid-related or whether you have non-acid reflux, regurgitation, or pressure-related symptoms that need a different approach.
Here, the microbiome angle also becomes practical. If reflux comes with marked bloating, belching, or abdominal pressure, treatment may need to go beyond acid suppression alone. Some patients benefit from evaluation for SIBO or other gut issues, and selected probiotic or supplement strategies may be discussed based on the full picture rather than used blindly.
When procedures are considered
A smaller group of patients may need procedural or surgical treatment.
That conversation usually comes up when medication is not controlling symptoms well, reflux keeps returning, there is a structural issue such as a significant hiatal hernia, or someone wants an alternative to long-term medication. Before that step, doctors usually want solid testing so the treatment matches the actual cause.
A common misunderstanding
People often assume that if a medicine dulls the burn, the whole problem is solved. Relief matters, but it is only part of good care.
The better question is why the reflux keeps happening. For some people, acid is the main issue. For others, the pattern includes impaired motility, regurgitation, delayed emptying, or gut microbial imbalance that increases gas and pressure. Sorting that out is what makes treatment more precise and far less frustrating.
Improving Gut Health for Reflux and GERD Management
Most standard reflux advice focuses on acid. Acid matters, but it is not the whole story.
A less discussed question is this: what if part of the problem starts lower in the digestive tract? In practice, many people with GERD also report bloating, pressure, belching, irregular bowel habits, or symptoms suggestive of small intestinal bacterial overgrowth, often called SIBO.
Why the microbiome may matter
Emerging evidence suggests that some people with GERD may also have microbial imbalance.
The Franciscan Health discussion of acid reflux and GERD highlights a 2025 meta-analysis reporting that GERD patients had 40% lower esophageal microbiome diversity and 3x higher SIBO prevalence compared with controls, with dysbiosis predicting non-response to PPIs in 28% of cases. The same source notes that Lactobacillus reuteri DSM 17938 has been shown to reduce GERD scores.
That does not mean every case of GERD is caused by the microbiome. It does mean that in some people, reflux may be worsened by a broader digestive imbalance.
How gut issues may feed reflux symptoms
This is the pattern I ask patients to consider:
- Bloating and gas can increase abdominal pressure
- Pressure upward may make reflux episodes easier to trigger
- Microbial imbalance may contribute to inflammation and poor tolerance of certain foods
- Persistent symptoms despite acid suppression may suggest there is more going on than acid alone
If your reflux comes with bloating after meals, excessive belching, or IBS-like symptoms, that clue is worth discussing with a clinician.
Practical ways to support gut health
These approaches are best used as complements to medical care, not substitutes for it.
Start with food tolerance, not food perfection
Fermented foods can be useful for some people, but they are not universal. Start small.
Examples include:
- Yogurt with live cultures
- Kefir
- Sauerkraut
- Kimchi, if spice is tolerated
- Miso, in gentle portions
If fermented foods worsen symptoms, stop and reassess.
Consider strain-specific probiotics
The strain matters more than the word “probiotic.”
If reflux overlaps with bloating or microbiome concerns, it may be reasonable to discuss a targeted option with a clinician, especially one containing strains studied for upper GI support. This digestive probiotic product review image reflects the kind of product category many readers compare.
{kind=link}
Track patterns for two systems, not one
Do not only record heartburn.
Also note:
- belching
- abdominal fullness
- bowel changes
- symptom timing after specific foods
- whether symptoms improved with smaller meals versus acid medicine
That fuller pattern can reveal whether reflux is part of a wider gut issue.
If acid suppression helps only partly, the next question should not always be “Do I need a stronger acid blocker?” Sometimes the better question is “What else in my gut is driving pressure, irritation, or poor response?”
Frequently Asked Questions About Reflux and GERD
Can I exercise if I have GERD
Usually, yes. Movement can support digestion and overall health.
The trick is timing and activity choice. Many people do better when they avoid vigorous exercise right after eating. A gentle walk after meals is often better tolerated than intense intervals, heavy lifting, or deep bending soon after dinner.
If workouts trigger reflux, look at three things: meal size before exercise, how soon you start, and whether the activity compresses the abdomen.
Can GERD improve without lifelong medication
Sometimes, yes. It depends on why the reflux is happening and how severe it is.
Some people improve with consistent changes in meal size, food choices, posture, body weight, and timing. Others need medication for longer periods, especially if inflammation is present. The goal is not to prove you can “tough it out.” The goal is to protect the esophagus while using the least intensive plan that still controls symptoms.
Is reflux during pregnancy different
Pregnancy changes the situation because hormones and physical pressure both affect digestion.
The Female Gastroenterology article on GERD versus acid reflux notes that 30-50% of pregnant women experience reflux, and it also describes evidence that pregnancy-safe probiotics such as Bifidobacterium bifidum BB-12 + L. rhamnosus GG reduced reflux episodes by 42% in RCTs.
That matters because many pregnant patients want non-drug support first.
Helpful first steps often include:
- Smaller meals
- Remaining upright after eating
- Avoiding very late meals
- Identifying personal trigger foods
- Discussing probiotic use with an OB-GYN or GI clinician
If reflux is frequent or severe in pregnancy, bring it up early rather than assuming you have to live with it.
If I only get heartburn sometimes, should I still care about gut health
Yes, especially if you also deal with bloating, irregular stools, gas, or food sensitivity.
Occasional reflux may stay occasional. But if upper GI symptoms cluster with lower GI symptoms, supporting overall digestive health can make your symptom picture easier to understand and manage.
When should I stop guessing and book an appointment
Book an appointment if symptoms are frequent, persistent, disruptive, or accompanied by warning signs such as swallowing difficulty, cough, chest discomfort, or regurgitation that keeps returning.
A short period of self-observation is reasonable for mild occasional reflux. A long period of self-treatment for recurring symptoms is not.
If you want practical, evidence-focused help with reflux, probiotics, fermented foods, and digestive symptom support, visit Healthy Gut Review. It offers reader-friendly guides that can help you compare gut health strategies and make more informed choices before your next shopping trip or doctor visit.